Release Of Information Template Mental Health
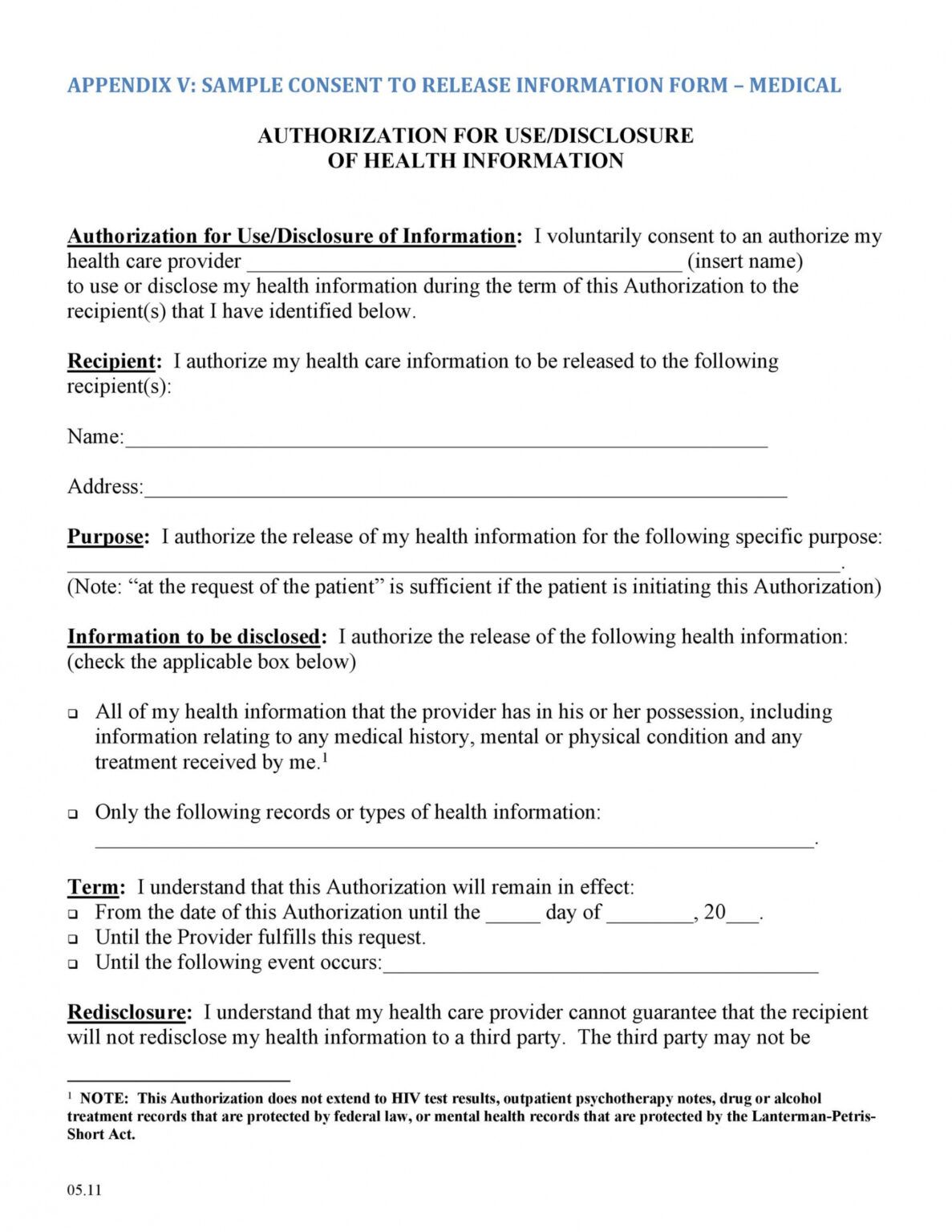
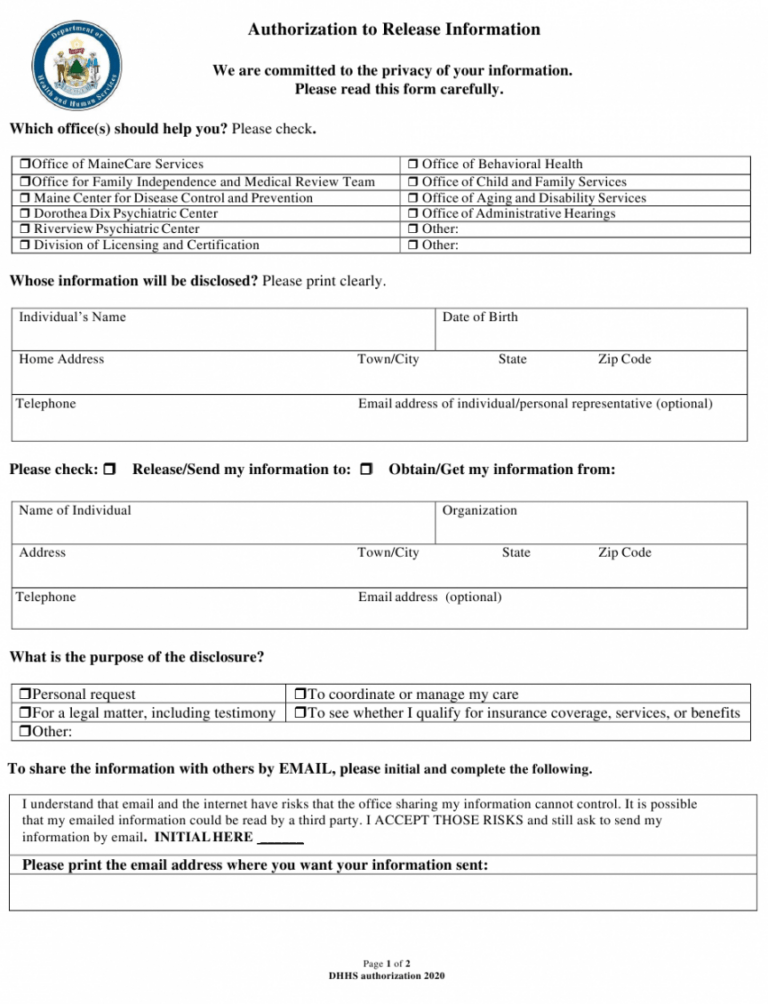
Release Of Information Template Mental Health - Addiction recovery management services unit; By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. Notice to receiving agency/ person: I have reviewed the above release of information form and refuse to authorize release of health and behavioral health. Meet your privacy obligations under hipaa with this authorization to release medical information form. To release, discuss, or disclose the following: Full treatment record including all health/mental health information [2 full treatment record excluding the following information: A mental health release of information form is a document a mental health professional provides to their clients to properly acquire the consent required to use or disclose health information for. Under the provisions of the illinois mental health and development disabilities confidentiality act, you may not redisclose any of this. Release of information form mental health Authorization for release/exchange of information this form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. The template is perfect for mental health. A mental health release of information form is a document a mental health professional provides to their clients to properly acquire the consent required to use or disclose health information for. Full treatment record including all health/mental health information [2 full treatment record excluding the following information: *** signature of witness who can attest to the identity of the authorized signatory is required to release any mental health or developmental disability information. Addiction recovery management services unit; Notice to receiving agency/ person: This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be shared. Full treatment record excluding the following information: Community notification of individual in custody early release; By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. Full treatment record including all health/mental health information Always stay on top of your patient's health concerns, and safeguard their details with. Authorization for release/exchange of information this form provides your therapist with. Community notification of individual in custody early release; To release, discuss, or disclose the following: *** signature of witness who can attest to the identity of the authorized signatory is required to release any mental health or developmental disability information. A mental health release of information form is a document a mental health professional provides to their clients to properly. A mental health release of information form is a document a mental health professional provides to their clients to properly acquire the consent required to use or disclose health information for. Notice of client’s refusal to release information: A mental health release of information form is a document a mental health professional provides to their clients to properly acquire the. Identify whether the form will be used to disclose, to obtain or to disclose/obtain (share) information and whom you are authorizing to perform this function. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. *** signature of witness who can attest to. Authorization for release/exchange of information this form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. To release, discuss, or disclose the following: I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all. Meet your privacy obligations under hipaa with this authorization to release medical information form. A mental health release of information form is a document a mental health professional provides to their clients to properly acquire the consent required to use or disclose health information for. Authorization for release/exchange of information this form provides your therapist with written permission to communicate. Identify whether the form will be used to disclose, to obtain or to disclose/obtain (share) information and whom you are authorizing to perform this function. Authorization for release/exchange of information this form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. *** signature of witness who can attest to the identity of the. Authorization for release/exchange of information this form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. Notice to receiving agency/ person: To release, discuss, or disclose the following: This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need. I have reviewed the above release of information form and refuse to authorize release of health and behavioral health. Under the provisions of the illinois mental health and development disabilities confidentiality act, you may not redisclose any of this. Authorization for release/exchange of information this form provides your therapist with written permission to communicate with other individual providers regarding your. Authorization to disclose protected health information to primary care physician (sample form) communication between behavioral health providers and your primary care physician (pcp). Notice of client’s refusal to release information: Under the provisions of the illinois mental health and development disabilities confidentiality act, you may not redisclose any of this. The witness cannot be the. I authorize the release of. Meet your privacy obligations under hipaa with this authorization to release medical information form. Kickoff announcement email purpose: I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that. By signing this form, confidential psychological and psychiatric information can be released to and/or discussed with the people or agencies listed below unless noted by exclusions or. Announce the start of mental health awareness month and share planned activities. To release, discuss, or disclose the following: A mental health release of information form is a document a mental health professional provides to their clients to properly acquire the consent required to use or disclose health information for. Identify whether the form will be used to disclose, to obtain or to disclose/obtain (share) information and whom you are authorizing to perform this function. Full treatment record including all health/mental health information [2 full treatment record excluding the following information: Authorization to disclose protected health information to primary care physician (sample form) communication between behavioral health providers and your primary care physician (pcp). Full treatment record excluding the following information: I have reviewed the above release of information form and refuse to authorize release of health and behavioral health. This template for release of information includes all of the information that you need to include and is clean, professional, easy, and fast to use. Release of information form mental health Always stay on top of your patient's health concerns, and safeguard their details with. Notice to receiving agency/ person: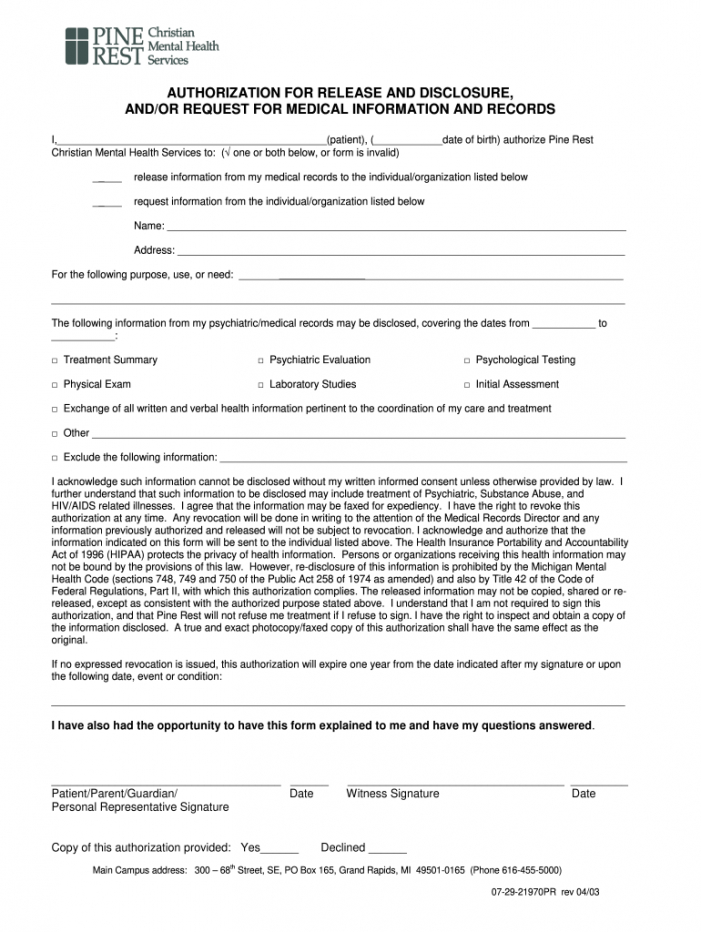
Mental Health Release Of Information Form Template

Mental Health Release of Information Form (Editable, Fillable
30 Medical Release Form Templates ᐅ Templatelab Mental Health Release
Mental Health Release of Information Form, ROI, PDF, Fillable, Editable

FREE 13+ Sample Release of Information Forms in PDF MS Word

Mental Health Release Of Information Form & Template Free PDF Download
Free Release Of Information Form Mental Health Template Doc

Release Of Information Form Template Mental Health
FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
FREE 9+ Sample Release of Information Forms in MS Word PDF
*** Signature Of Witness Who Can Attest To The Identity Of The Authorized Signatory Is Required To Release Any Mental Health Or Developmental Disability Information.
The Purpose Of This Disclosure Of Information Is To Improve Assessment And Treatment Planning, Share Information Relevant To Treatment And When Appropriate, Coordinate Treatment Services.
This Template Can Be Used To Coordinate The Release Of Confidential Information During A Client's Transition Of Care Or Other Cicrumstances Where Private Records Need To Be Shared.
Community Notification Of Individual In Custody Early Release;
Related Post: